Bilaga om Corona, SARS-CoV-2 och COVID-19
2020-06-06
Our work has been somewhat affected lately, during the pandemic. We have received requests for testing equipment for the control of virus separation and through this also got into investigating the market for medical water and medical equipment. (Our technique separates viruses without difficulty.)
The discovery that many deaths from COVID are related to underlying lung problems from air pollution has given greater urgency to the work of purifying combustion gases using water scrubbers. In May/June our doctoral student, Imtisal, will present her highly interesting reports at the Högdalen power station outside Stockholm and at the Bristaverken in Märsta. Improved combustion gas purification will now be one of our priorities.
The work of purifying well water in India has unfortunately come to a complete standstill during the pandemic, as it was impossible to install the heat exchangers we needed in order to convert from waste heat operation to solar energy. Instead, we have focused on our major project for the desalination and purification of water using solar power, which we will shortly report on.
While working on issues around viruses and COVID we have encountered a fair amount of startling facts of general interest that I will share in the following compilation. The virus from Wuhan in China was said to be unusually infectious and unusually lethal. The WHO declared it a pandemic. Shortly after this, country after country began introducing restrictions and quarantines.
PANDEMIC
In the early stages of each wave of influenza, very many die among those who are, from a medical point of view, the most delicate and vulnerable.
In Lombardy and Wuhan, these were individuals whose lungs had already been destroyed by air pollution.
In Sweden, they were individuals who were already close to death in understaffed care homes.
In other places, a combination of air pollution, malnutrition, and overcrowding played an important part.
If you then assume that the mortality rate – i.e. deaths per person infected – will remain at the same level as during the early stages, then you are looking at a pandemic.
If the WHO (and others) had kept a cool head in that situation they might have discovered that it was a question of a relatively normal influenza. Perhaps one of the worst, perhaps one of the mildest. It would have been difficult to know at that stage. It is only now that we are beginning to get the answers.
Statistics from Sweden about COVID-19. A minor increase in death rate in 2020
Daily and weekly figures for the transmission of the SARS-CoV-2 virus and its consequences as reported by authorities and media have this far been speculative and confusing.
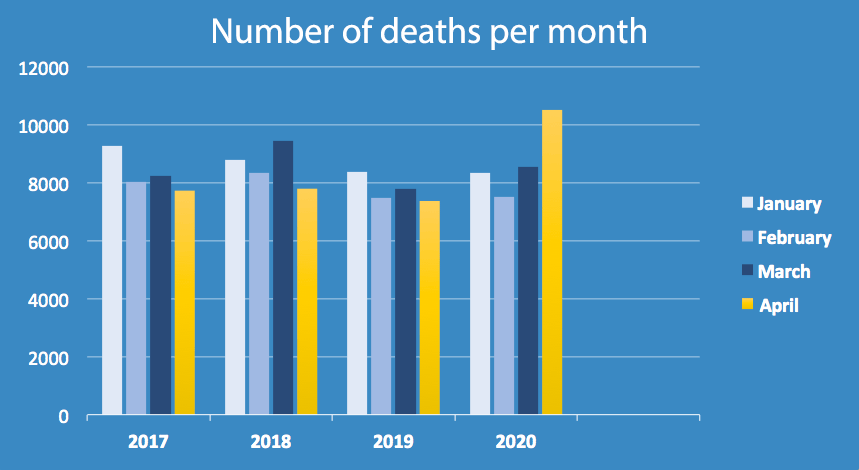
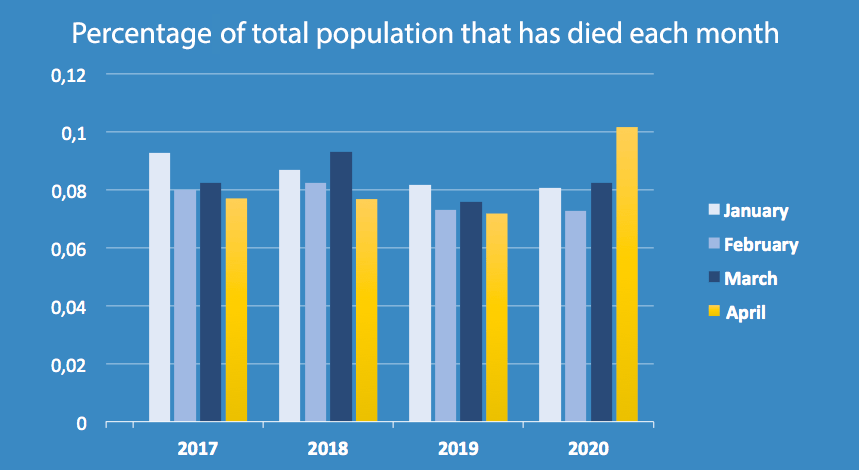
Official Swedish figures that were released on the 5th of June 2020 are still preliminary but are based on reported and scrutinized figures. The first table shows the death rate for comparable months. The second table shows the total number of deaths per month. Both are based on the published official statistics from Statistics Sweden.
Figures for May 2020 will be available in the beginning of July.
©Scarab Development AB, June 5, 2020
All the time there was a storm of frightening numbers and forecasts in mass media. An apocalyptic mood was created. However, we still – four months later – do not know how infectious the virus actually is. Nor do we have any certain information about mortality rates. Our facts consist of contradictory information and rumour. Our overall knowledge is at the level of “terribly many” people dying and that it “can hit anyone”. Sometimes Sweden seems to be doing well. At other times it is said that the mortality rate is higher in Sweden than anywhere else. The authorities speak of data lag. The fact is that no “daily” numbers are correct.
It seemed as if we could - as if by magic - retrieve daily data on daily infections and daily deaths in all countries in the world. Many countries do not even know how many inhabitants there are. In Sweden, we probably know – forgetting those who are undocumented. But we do not exactly know each day how many have died from a specific cause. Knowing how many have been infected by a specific virus on a specific day is in practice impossible.
WHAT ACTUALLY IS COVID-19?
About 90,000 people die each year in Sweden, i.e. nearly 250 per day or about 7,500 a month. Most of those who die are naturally older or have multiple illnesses. These people are also particularly vulnerable to virus infection. It is therefore important that they are not exposed to infection. But when the person eventually dies it is not always easy to establish the immediate cause of death.
COVID-19 is a concept created by the WHO early in 2020 and it refers to various types of severe illness in people infected with SARS-CoV-2. The Swedish Public Health Agency uses the following definition ”COVID-19 is the official name of the illness caused by the new coronavirus SARS-CoV-2 (SARS-coronavirus-2). COVID-19 means coronavirus disease 2019.”
SARS-CoV-2 is the virus that created the pandemic in 2020.
Corona is the name of a group of viruses that in humans normally cause a cold with a sore throat and a cough, and sometimes pneumonia. The symptoms are usually mild but might occasionally cause or aggravate a deadly disease. We call it a cold, or a runny nose, sometimes influenza. There are no approved vaccines for these viruses and no drugs that cure them. Medicines might possibly alleviate or shorten the course of the illness.
The first coronavirus to infect humans was discovered in the 1960s. New viruses within the group are SARS-CoV in 2003, HCoV NL63 in 2004, MERS-CoV in 2012, and SARS-CoV 2 in 2019.
Mix-up of cause and effect
Initially, mass media talked about ”Corona”. The virus itself is called ”Severe acute respiratory syndrome coronavirus 2” (SARS-CoV-2). Before long, the WHO had coined a new expression: COVID-19 (Coronavirus disease 2019). This is the name of the illness that the virus is considered to be causing.
But later on, the WHO mix up virus and illness, for instance when they write “people infected with the COVID-19 virus”. Here, the name of a virus is mixed up with the name of an illness that the virus is considered to be causing or contributing to. ”Coronavirus COVID-19” becomes a concept that will be used by experts as well as mass media.
Here is the WHO’s information from a period when they had not yet mixed up the concepts, downloaded 2020-05-14
What is COVID-19? COVID-19 is the infectious disease caused by the most recently discovered coronavirus. This new virus and disease were unknown before the outbreak began in Wuhan, China, in December 2019. COVID-19 is now a pandemic affecting many countries globally. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/question-and-answers-hub/q-a-detail/q-a-coronaviruses
Coronaviruses are a large family of viruses that may cause illness in animals or humans. In humans, several coronaviruses are known to cause respiratory infections ranging from the common cold to more severe diseases such as Middle East Respiratory Syndrome (MERS) and Severe Acute Respiratory Syndrome (SARS). The most recently discovered coronavirus causes coronavirus disease COVID-19. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/question-and-answers-hub/q-a-detail/q-a-coronaviruses
In research, as well, the concepts are beginning to be mixed up. After first comparing SARS-CoV-2 with other viruses, the researcher writes “… through analysis of COVID-19 (SARS-COV-2)” and finishes further along with ”…transferability is higher for COVID-19 than for SARS…” The virus does not just cause or contribute to the illness but has been transformed into the illness. Srijan Haldar, April 27, 2020 http://adamasuniversity.ac.in/is-sars-cov-2-more-deadly-than-sars-cov/
UNICEF mixes up the concepts: “Cleaning and hygiene tips to help keep the COVID-19 virus out of your home”. https://www.unicef.org/coronavirus/cleaning-and-hygiene-tips-help-keep-coronavirus-covid-19-out-your-home And the Public Health Authority of Sweden also mixes up the concepts: “Decisions and guidelines in the Ministry of Health and Social Affairs’ policy areas to limit the spread of the COVID-19 virus”. https://www.government.se/government-policy/the-governments-work-in-response-to-the-virus-responsible-for-covid-19/
Mix-up of cause and effect
On a death certificate, the doctor can mark different alternative sicknesses that have contributed to or caused the death. The immediate cause of death might for instance be “Breathing problems”, “Metastases”, “Heart failure”, “Sepsis”, “Internal bleeding”, etc. The WHO has now decreed that there must also be a box for COVID-19 and one box for a notation “Probably COVID-19, not verified by lab test”. The risk of a mix-up of an illness and the cause of the illness is therefore high even in this serious and ultimate context.
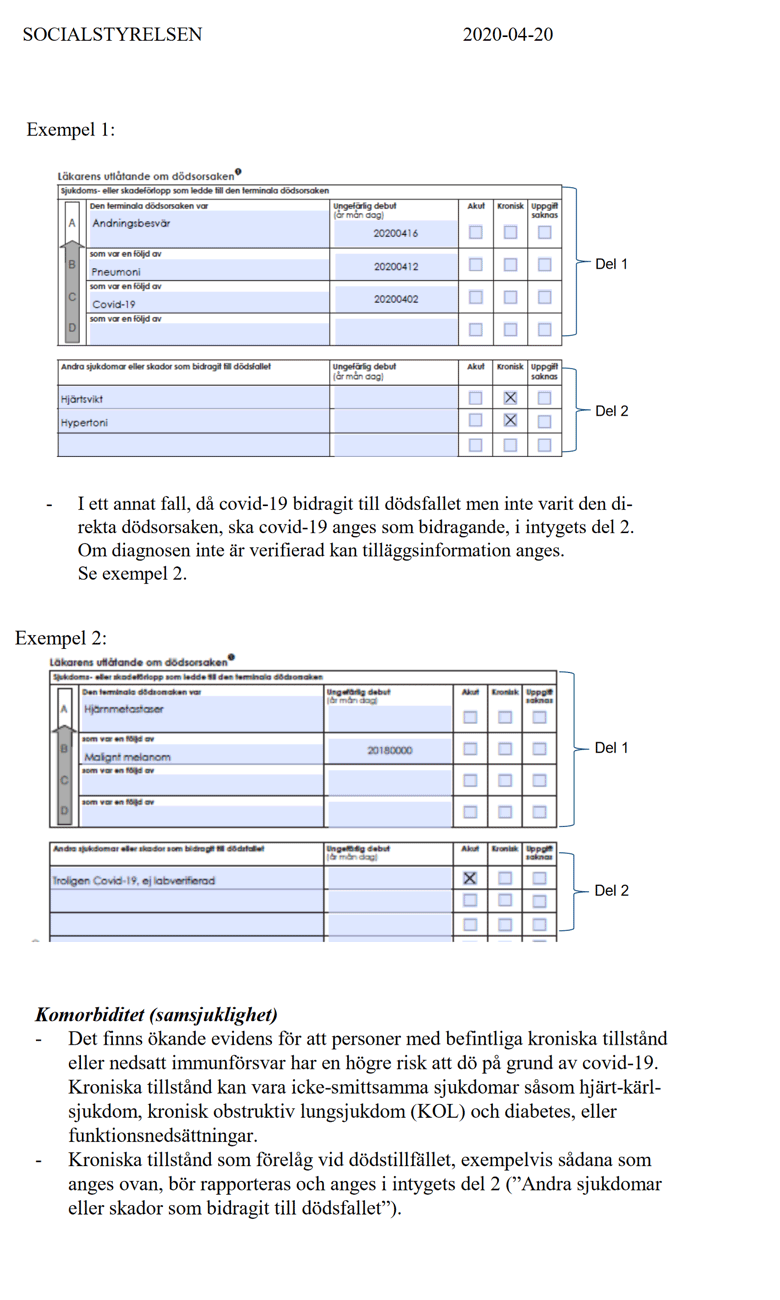
The WHO’s upgrading of death certificates has had the effect that practically every death can be classed as COVID-19 provided that the SARS-CoV-2 virus is or can be suspected of being involved.
A large number of previously known fatal diseases are therefore labelled and registered as COVID-19 as soon as there is confirmed or suspected or probable infection by SARS-CoV-2. Confirmed COVID-19 is used if the patient has tested positive for SARS-CoV-2, ”suspected” COVID-19 if the patient has symptoms that resemble influenza and ”probable” COVID-19 if the patient shows changes ”compatible” with COVID-19. This naturally generates a large total number of deaths from COVID-19. This approach has also spread to the general public. A friend of mine told me in great distress that her friend had died from COVID even though she was only just fifty. She also told me that her friend had recently been treated with radiation and chemotherapy for cancer. Did she then die from cancer or from COVID?
What are the symptoms of COVID-19?
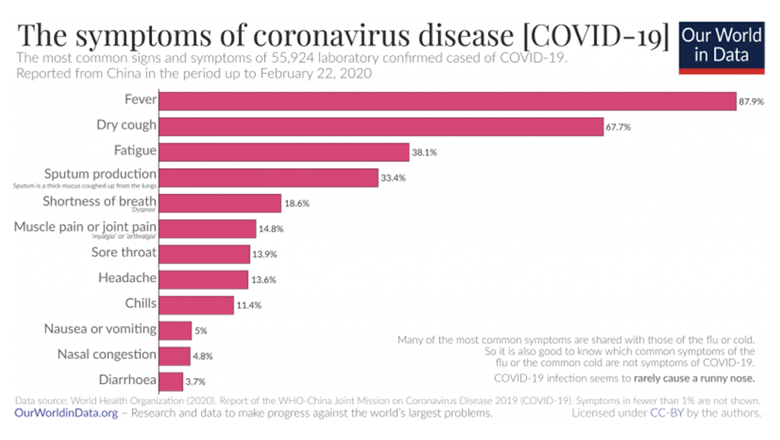
Already at an early stage, a study from China published in JAMA (Journal of the American Medical Association) showed that the typical symptoms of “COVID-19” resembled the symptoms of influenza and seemed to start with a high temperature, followed by a dry cough.
In some patients – particularly the elderly and others with other chronic health conditions – pneumonia, chest pain, and breathing difficulties might develop after a week. About 20 percent of patients needed hospital care. The ”COVID-19 infection” appeared rarely to cause a runny nose, sneezing, or a sore throat. These symptoms were only noticed in about 5 percent of patients. A sore throat, sneezing and a blocked nose are usually signs of a common cold.
This description of symptoms seems to remain valid.
It is difficult to see which among the symptoms listed above could be the cause of death. It can be assumed that the most common cause of death in COVID-19 is not the virus infection as such but what is known as “underlying illness”.
Fever, dry cough, fatigue, sputum in the throat, shortness of breath, muscle pain, sore throat, headache, chills, nausea, vomiting, blocked nose, and diarrhoea. It is hard for a layman to see what could be fatal other than shortness of breath. These were the symptoms observed in China. In Sweden, the symptoms are the same or similar. But it has also been reported that it is not only those with weak lungs who are the largest at-risk group (as in Wuhan) but people with serious illnesses such as high blood pressure, heart failure, and diabetes. Is it then really the same illness? In these cases, one should probably say that the effects of the SARS-CoV-2 virus exacerbate the illness, but the patient dies from the original illness. Nevertheless, the death certificate will probably say COVID-19 and in official statistics, this will probably count as death due to COVID-19. At any rate, the newspaper headlines will count it as COVID-19.
Is COVID-19 an illness?
COVID-19 is not an illness in the traditional sense, like tumours, diabetes, etc. And it is not an ordinary cause of death like a ruptured aorta, heart arrest, blood clot, sepsis, etc. COVID-19 is a tick box on the death certificate to indicate that SARS-CoV-2 plays a part. Or that you can suspect that SARS-CoV-2 plays a part, or that there is a ”connection”, i.e. that you guess that SARS-CoV-2 plays a part. The doctor ticks the box and mass media gratefully accepts. The person died from COVID-19!
Of course, the virus may be involved. It weakens the body. It can accelerate death. But it is one player among many and rarely the most important. Perhaps just the caddie.
It would seem fairly likely that if the doctor puts a tick for COVID-19, then COVID-19 will appear in the statistics one way or another. It would be difficult after the event to separate out which of the patients dying from COVID died from SARS-CoV-2, and which died from different causes.
Some researchers say that it will be years before we have all information on the table. But some information will probably never get out. One idea that has been put forward is to compare the number of deaths from COVID-19 with the number of deaths from influenza in other years. But while an individual dying from heart failure this year and who has tested positive for SARS-CoV-2 may be recorded as dead from COVID-19, somebody who had influenza and died from heart failure last year is most likely to have been recorded as dead from heart/vascular disease. Earlier records usually do not include influenza as a cause of death. You die ”with” influenza, not ”from”.
Perhaps it does not matter too much to the individual doctor what the death certificate says. But to the authorities who have invested a great deal of prestige in fighting COVID-19 it can be of importance. And if the pharmaceutical companies manage to get a look-in, then COVID-19 is of course preferable to any other illness since there is a lot of money to be had for such research right now.
During a period of less than six months, an enormous quantity of scientific articles about COVID 19 has been published. On 30 May, I got 54,300 hits in Google Scholar on COVID-19 for articles published in 2020. Most of them probably end with the usual final flourish of scientific articles – more research is needed.
At the same time, there have no doubt been thousands of applications handed in for grants for the development of treatments and vaccines. All of these researchers will of course swear that COVID-19 is an entirely new and unknown illness which moreover is extremely dangerous. But let us hope that the research results are more evidence-based than the drive of the pandemic in mass media has been. It is remarkably casual for the WHO not to probe deeper into the effects of the virus but instead, all in a rush invent an entirely new illness with an entirely new previously non-existent diagnosis and in addition prescribe a new box on the death certificate for the new illness. In this case, medical science does not give the impression of being an exact science.
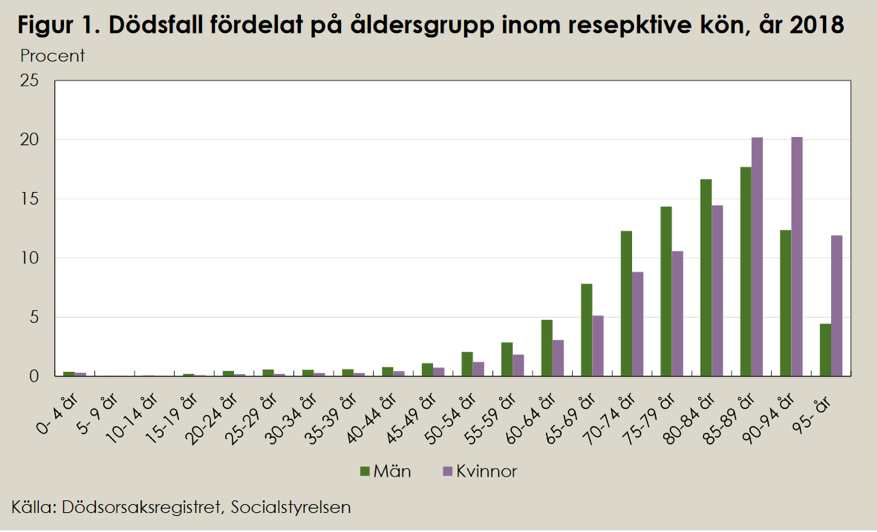
Much has been written about COVID-19 particularly affecting older people. This should not be especially remarkable. This is what the age distribution for deaths looked like in a normal year, 2018.
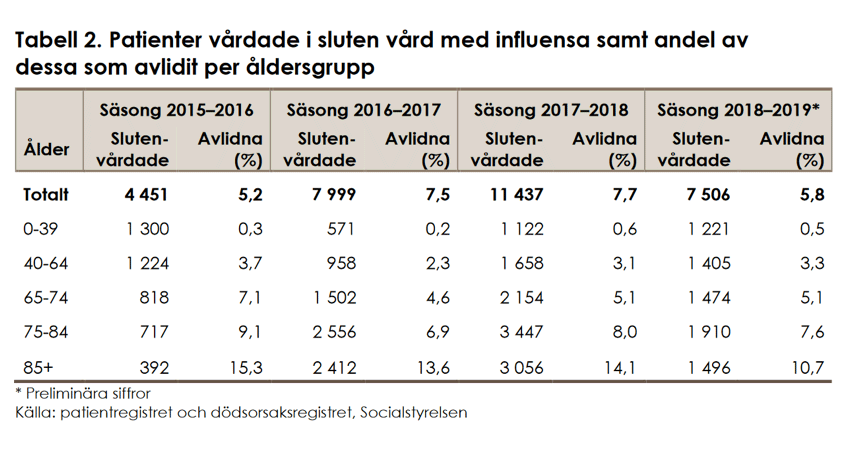
Both of the above tables can be found at https://www.socialstyrelsen.se/globalassets/sharepoint-dokument/artikelkatalog/statistik/2019-9-6298.pdf
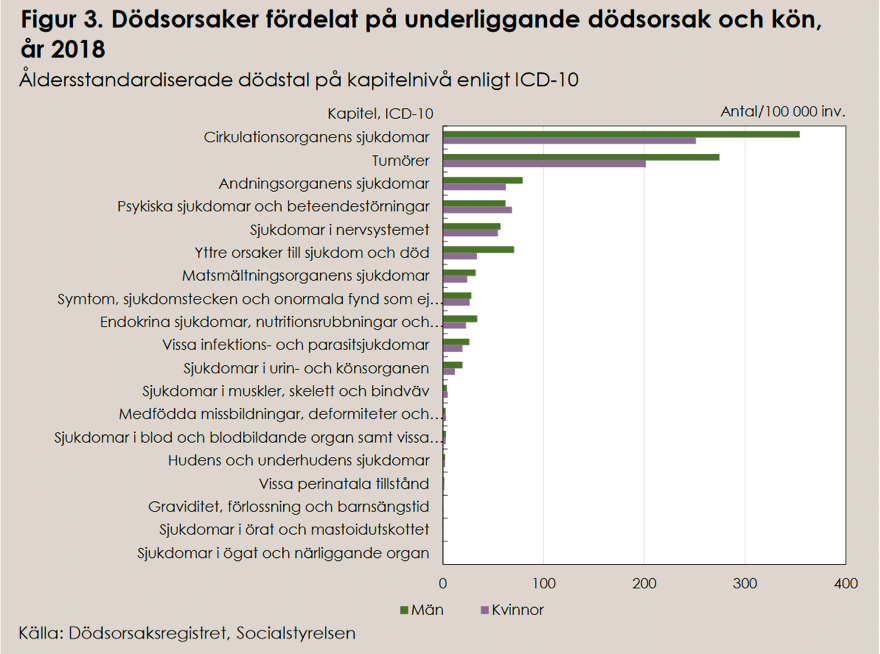
Here we can see the causes of death in 2018. You may wonder if the National Board of Health and Welfare will squeeze in COVID-19 as an entirely new cause of death in the statistics for 2020? Or if it will be listed under illnesses in the respiratory organs or under the other contributing causes of death that may have been noted on the death certificates. Note that there is no ”influenza” in the table. Of course, many people have influenza when they die. Influenza leading to pneumonia is a common cause of death. But you do not say that a person dies from influenza, just as you would not say that a person died from a cold or a runny nose. But when mass media talk about COVID-19 they most often say that the person is suffering from/dies from CORONA-19. That is slightly different.
Note that the National Board of Health and Welfare writes ”with” influenza and not ”from” influenza.
”WE MUST PROTECT OUR OLDER PEOPLE”
Most of the political and medical measures implemented in Sweden and most other countries during the Corona pandemic have been justified by “we must protect the elderly”. But have we done this?
Thomas Lindén at the National Board of Health and Welfare writes in the Aftonbladet newspaper of 21 May 2020: ”You can also express it as that of 100 people over 70 living in accommodation for the elderly, two have died from COVID-19. But the impression given is that it is basically handing out a death sentence to place your elderly family members in care homes.”
The majority of older people who fall ill with COVID-19 survive. Statistics from the Stockholm Region show that seven out of ten patients on geriatric wards (care for older people) have recovered after falling ill. There are similar results internationally.
Therefore, COVID-19 is less of a risk for older people than what mass media accounts suggest. On the other hand, a report from the National Board of Health and Welfare shows that the care homes are perhaps not very good in themselves.
You can see that the number of places in care homes has been reduced considerably during recent years. In 2019, it was reported by 127 municipalities that they had a deficit of special accommodation for older people. Those who arrive in the care homes are often already very old and with failing health when they move in.
Waiting times have become longer. During 2018, the average waiting time was five months. In relation to the needs and life expectancy of the elderly, this means that they have a relatively long wait before moving to special accommodation. Sometimes they die before they get a place and sometimes they are already so ill that they cannot move in when they are finally allocated a place but move to short-term accommodation or receive added support at home. Those who get a place often die after a short period in the care home. The average stay in special accommodation is about two years.
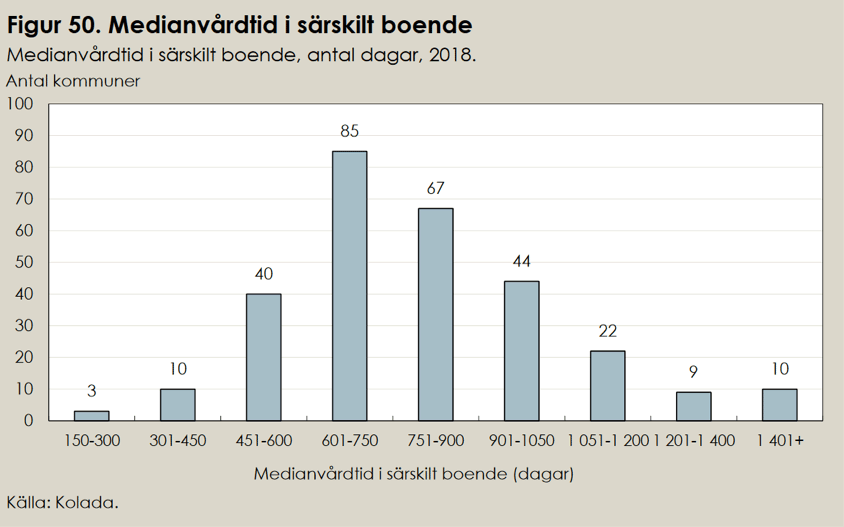
The three municipalities with the shortest time have an average stay of 150–300 days. The average stay nationally is 720 days. Six months after moving to special accommodation an average of 20 percent of the new arrivals died: 24 percent of the men and 18 percent of the women. This was before COVID-19.

Eighteen months after moving in, 51 percent of the men and 61 percent of the women are still residents in the special accommodation. Thus, half of them die within one and a half years.
Numbers and tables are from Vård och omsorg om äldre, Lägesrapport 2020 [Care of the elderly. Situation report 2020], National Board of Health and Welfare https://www.socialstyrelsen.se/globalassets/sharepoint-dokument/artikelkatalog/ovrigt/2020-3-6603.pdf
Older people in need of care are, as we can see, already in a dire condition. Many of them have worked for 40–50 years in the community. It is a shame that we should have to squeeze the resources for their final one or two years of life.
If death rates for the elderly in care homes are unusually high right now, this is not just because the elderly have been infected by the virus via their grandchildren and great-grandchildren. Perhaps the sadness of not being allowed to see their children, grandchildren, and friends during the last months or the last year of their lives is of equal importance.
The reason old people in Sweden have been particularly badly affected by the virus epidemic might be that Sweden is recognised as being at the forefront of the application of the ”new public management” concept, which was launched internationally by researchers, consultants, and lobbyists in the early 1990s. New public management can also be expressed as ”New management of the public sector”. In Sweden, concepts such as performance management, target management, and programme budgeting have been used. It is an umbrella concept for reforms of the organisation and management of the public sector and intended to make it more efficient.
The concept has a counterpart in the private sector, the concept of ”lean management” which is an effort to maximise customer benefit and at the same time minimise the waste of resources through various types of efficiency improvement and rationalisation. It has been adopted with success by Toyota and today it is probably generally accepted as an objective for all industrial operations.
The fundamental purpose is to reduce administration and bureaucracy in order to achieve more efficient use of resources – to cut away fat and excess flesh.
When the politicians after much investigation decided to introduce performance management, it was the municipal authorities that were given the task of implementing the rationalisation measures that had been decided on.
But then Parkinson’s well-known sociological laws kicked in, especially the one stating that every manager in an administration strives to increase the number of administrators under him or her so as to expand his or her importance and power. This tendency is kept under control in private businesses through the demand for profit, but in the public sector, it is able to flourish. Therefore, numerous consultants and middle managers were employed to implement the new reforms. At the same time, another of Parkinson’s laws kicked in, the one that says that an administrator’s work expands to fill the available time. The municipal administration ended up working at full speed to implement the rationalisation measures that had been decided on and grew rapidly in line with these two Parkinson’s laws.
Cyril Northcote Parkinson (30 July 1909 – 9 March 1993) was an English history professor who wrote about sixty books, the best known of which appeared in 1958 under the title ”Parkinson’s law and the pursuit of progress”. It is written in a tongue-in-cheek manner but is based on interesting research. His theories met with acclamation and success during the 1960s but today they are more or less forgotten. But well worth reading. One of his humorous examples (he was basically a naval historian) was that if the development that he had studied were to continue the English navy would before long have more admirals than ships. This was at the time regarded as very funny and was assumed to be a case of ironic exaggeration. Even if the prediction has not entirely been fulfilled the identification of the trend was correct. For example, the US navy currently has about 225 admirals – and about 260 warships in active service.
The purpose of rationalisation was of course greater efficiency, which looked at from another perspective means savings. With administration turning out to require ever higher expenditure there was only one way of reaching (performance management/target management) the stated savings targets and that was to make cutbacks in the activity itself.
Examples are hardly necessary. All Swedes, and in particular all public sector employees, have seen an increase in paperwork while resources for the activity itself have had to take a back seat. On the rare occasions when I have had to personally attend A&E it has hardly looked like in the TV series where staff run around the stretchers carrying drip bottles. It is more likely that a large portion of the staff are sitting working at their computers while all except the most critical patients are sitting or lying in the corridors, patiently waiting.
Looking only at care for older people it is crowded with decision-makers and administrators while the number of care beds has been minimised, staffing levels have been reduced, staff training has been allowed to lapse and resources for food, materials, and cultural activities have been reduced to a minimum. The situation for care at home, which is the alternative for those who cannot get a place in special accommodation, is similar.
The combination of performance management and Parkinson’s law has created an organisation with sky-high salaries at the top, increasing numbers of highly paid middle managers, fewer doctors, fewer nurses, fewer nursing assistants, while orderlies have been completely rationalised away. This development has turned into a self-playing piano. The more the activity underperforms, the larger is the number of consultants and middle managers believed to be needed in order to improve the situation. As business people and shareholders, we might be safely out of it. But at least for my own part, I want to live in a country where all old people receive efficient and dignified care delivered by a human hand. We need more care beds and more care staff. Not more bureaucrats.
THE ROLE OF MASS MEDIAL
The power of mass mediat
Surprisingly, “the whole world” immediately accepted the idea that the new SARS virus (SARS-CoV-2) was an unusually deadly virus that was spreading unusually aggressively. The number of infected people and deaths could be found in all headlines. All mass media in the world were daily, for weeks and months, emphasising how unusually dangerous this pandemic was. How could they know?
In country after country, urban myths were created about how people were lying dead in the streets, how mass graves were prepared and how coffins were stacked in various peculiar locations. Similar tales were also reported by mass media about countries with hardly any infections. The reports came from well-established news agencies like TT and Reuters. Was any of it true?
None of the numbers flying about in international mass media – serious or not – have had any firm basis. For obvious reasons, there have not been any completed statistics. It is not possible to develop data that quickly. Therefore anyone has been free to communicate “facts” and make predictions.
Information pages on the Internet seem to update the spread of infection and numbers of deaths with a delay of just one second.
Most things about COVID-19 are still unknown How did the new SARS virus originate? How infectious is it? How great is its mortality rate? When might it be over? How many are asymptomatic carriers? For how long are you infectious once infected? Are there many virus strains or just one? Are the tests reliable? What is the risk of the present virus mutating and becoming even more aggressive? Or less harmful? Will there be a second wave? At what percentage do we reach herd immunity? Is herd immunity at all possible? Do antibody tests work? For how long are you immune if you test positive for antibodies? For how long are you immune under herd immunity? Do other tests work? For how long does the virus survive outside the body? How significant is the size of the dose you take in? Can the virus spread through air, through contact, through someone’s breath, or only through droplets? All of this has been discussed in mass media, but this does not appear to have been in order to inform but to create headlines. To sell copies, like serious journalists have a habit of saying about the evening papers. Politics and the authorities have had to react to the mass media debate.
Mass media logic
The number of media outlets and channels is rapidly increasing. The fight for viewer numbers accelerates. This leads to overstating, oversimplification, polarisation, concretisation, personification, intensification, and stereotyping. This is what media research refers to as mass media logic and it is a dangerous development that has been accelerated during the Corona panic.
Nothing suits the mass media logic better than a worldwide panic. This is then seasoned with the spice of deadly serious – and just as poorly founded – rhetoric of experts and politicians fighting for airtime on the daily television news programmes. You get the impression that the editor told them: ”Say something startling, or you won’t be invited next time…”. No matter how calm and sceptical you are, the endless flow of false numbers and ominous predictions is frightening. Politicians are forced into measures that create a disaster far greater than the original virus infection. When none of the disaster headlines (e.g. collapse of intensive care) turn to reality and when preparations for the disaster (e.g. field hospitals) remain unused, the politicians will say that it was thanks to their determined interventions that we escaped.
The initial great upsurge of hysteria can be explained by poor management of statistics. But why has it continued? If you count deaths at the start of an epidemic, when many of the weakest in the groups at risk die, and there are no figures for how many have been infected, then there will be many deaths per infected person. If you then say that it is a very infectious virus the curve goes through the roof.
People panic. Perhaps it was not intended. There is no conspiracy. But that is how it works. These are the consequences of the mass media logic.
When calmer counsel arrives and more relevant numbers become available the mortality predictions are reduced from, say, six percent to perhaps three percent down towards one percent. It is likely that the mortality rate will end up at nothing higher than 0.1 percent (of those infected). Even this might turn out to be too high. Some researchers now suggest even lower numbers for COVID-19. Ten times lower. It ranges between 10 and 0.01 percent.

Mass media are dependent on being noticed. Here is a typical example of mass media logic. A majority of middle-aged and older people have what doctors consider to be too high blood pressure. This does not have to mean that you are in an at-risk group. But it might mean this!
The problem of statistics
Where do the daily data on mortality originate? The least you can say is that they are uncertain. How do you produce the eye-catching forecasts? Where does the input come from?
It is part and parcel of the nature of statistics that it is difficult to produce correct numbers and mass media would require unsurpassed self-control not to exploit this. Statistics do not appear spontaneously. There is a need for work that has to be planned and implemented in a professional manner. The primary requirement is that this is carried out correctly. Another just as important aspect is the context in which the statistics are used and their purpose. At every stage, there are sources of error. Here are some of the stages of the work:
Problem formulation. What is the purpose? Identification. Which data are essential? Method. How is information to be collected and processed? Collection and compilation of statistics are always time-consuming and prone to errors needing analysing. Evaluation. How reliable are the sources and the collection methods? Processing. Converting facts to usable knowledge. Interpretation of collected data is the next problem. Presentation. The authorities might either be interested in keeping the numbers down or in exaggerating them. Mass media usually want to exaggerate. Understanding. Ensuring that the recipient can assimilate the information. Numbers can be dangerous. Consider how many are suffering from the consequences of the Corona hysteria. And consider how many have experienced sleepless anxiety as soon as they or their families have shown symptoms of influenza. Truth would lessen the anxiety. And in this way probably also make the illness milder and reduce the deaths. But it is no part of mass media logic to accept responsibility for consequences. Mass media themselves consider that their mission is to convey the truth. And they often believe that this is what they do.
WHO CAN YOU TRUST?
An international foundation at the Johns Hopkins University outside Washington DC provides a continuous evaluation of pandemic preparedness in different countries.
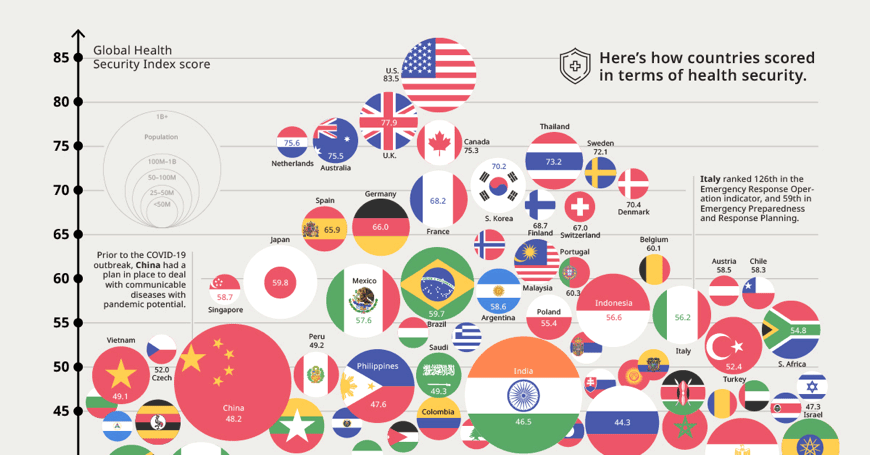
The Global Health Security (GHS) index is the first comprehensive evaluation of health security and preparedness in the countries of the world. www.ghsindex.org Higher up means higher total preparedness for meeting threats to the health of the population. The size of the circles shows the size of the population in each country.
The Corona pandemic has upended the pyramid. The two countries believed to have had the highest level of preparedness in 2019, i.e. the US and Britain, are those that have probably suffered most in 2020.
Here you can see who is leading the work that results in the index: https://www.ghsindex.org/about/#International-Panel-of-Experts
The practical work is carried out at the John Hopkins University, where there is an institute that has been engaged in epidemiology research since the 1990s Johns Hopkins Center for Health Security. Much of the current mass media information about COVID-19 comes from this institute. https://www.centerforhealthsecurity.org/who-we-are/history/
There must be a systematic error in the comprehensive and expensive preparedness analysis. A guess is that the error consists of giving great emphasis to the development of medicines and vaccines in the analysis, while less emphasis has been given to social conditions such as health care, care of the aged, forms of housing, and poverty.
TO CONSIDER IN RELATION TO COVID-19
Mass media reports might give the impression that the infection is evenly distributed around the world. Many were worried that the effects would be even worse in poor countries with limited resources for health care. As yet nobody can know how it will develop, but from this picture in the Financial Times it does not look like it.

Please note that the picture does not show the spread of the SARS-CoV-2 virus. If this had been the case it would have started much earlier. It shows the number of deaths according to the new diagnosis COVID-19. There might be many explanations of why COVID-19 has until now looked like a bigger problem in Europe and the US than in the rest of the world. It might be because the spreading of the infection actually began in Europe or the US and not in China. It might be because many countries in the rest of the world have poorer or slower reporting or that they have not conformed with the WHO’s new guidelines for diagnoses. At any rate, it is remarkable that there are not greater numbers of deaths in China where it all started or in populous and poor countries like India and Indonesia. The Financial Times statistics definitely do not tally with all mass media reports from more or less exotic locations where people are lying dead in the street. Where they are digging mass graves. Where the mortuaries are full, and it is difficult to find premises where the coffins can be stacked.
Is COVID-19 a lifestyle illness?
Might CORONA-19 be a mainly Western problem?
The graph from the Financial Times shows that COVID-19 has, at least up until now, hit rich societies – welfare societies – hardest. We know that the by far largest group of people at risk consists of older people with “lifestyle illnesses” such as obesity, diabetes, and heart and vascular diseases. This might explain the remarkable picture from the Financial Times where the US seems to have been worst affected, followed by Western Europe.
What is the role of air pollution?
In my previous letter, I wrote that the WHO calculates that air pollution causes more than four million premature deaths each year and that you might therefore suspect that air pollution is a strong contributory cause of what we are calling the Corona pandemic. Wuhan and Lombardy, both badly affected, are also known to have high levels of air pollution. It turns out that other WHO sources state that 9 million deaths each year are caused by air pollution. These are of course uncertain numbers. Air pollution is probably a more significant contributing cause than the virus.
What to do?
I wrote about face masks in my previous compilation.
It is completely absurd that authorities, governments, and experts demand the use of face masks for private individuals, even though there is no science supporting the demand, no evidence, and common sense sees much that argues against it.
There is just as little evidence in favour of what is now universally known as lockdown. The concept of lockdown has traditionally been used in cases of riots in prisons when the prisoners are locked into their cells. It is also common to use curfews to calm down entire communities. There is a tradition of isolating infection carriers by putting them in quarantine. But putting healthy people in lengthy quarantine in order to protect them from infection does not seem to have been tried before. The effect is therefore entirely unknown, and the procedure has no scientific backing. Can it really be justified? There is certainly much to suggest that lockdown ”flattens the curve” which was the obvious argument in most countries. But did it work? Was it needed?
The WHO and the pharmaceutical companies are promising that we will be able to fight COVID-19 with the help of new medicines and vaccines. In certain other cases, vaccines have been successful, but sometimes they are ineffectual and sometimes they are dangerous. We also know that we have not managed to develop effective medicines against influenza, and we have not found any vaccine against HIV in spite of spending billions over 35 years on just this.
The problem with COVID-19 is said to be that it is caused by an entirely new virus – SARS-CoV-2 – and that developing vaccines takes time. The same people also usually say that the viruses mutate very quickly. What suggests that the vaccine will be effective next year – on the mutated virus?
Now researchers, pharmaceutical companies, international organisations and politicians are promising to bring out vaccines within six months (when the pandemic has already blown over?). Politicians have already allocated billions. The number of new research efforts and new companies is growing. Irrespective of whether the search for new vaccines and new medicines is successful or not there are many other things that we can and should do:
- Reduce air pollution to reduce pulmonary illnesses
- Improve animal husbandry so that it does not provide fertile soil for new types of virus
- Improve the care of older people
- Adequate resources for the health service
- Eliminate lifestyle illnesses by supporting health maintenance instead of medicines
- Improve immune response through better diet and exercise.
It is not difficult to see the way ahead. But will we choose it when the Corona panic is finally over?